Beta-Blocker Safety Calculator
Enter your asthma control and cardiac needs to see if cardioselective beta-blockers are safe for you. Based on clinical guidelines and the latest research.
- 1. Rate your asthma control (0=worst to 100=best)
- 2. Select your cardiac indication severity (1=least to 5=most severe)
- 3. Choose your beta-blocker type
0=Uncontrolled (frequent ER visits, rescue inhaler >4x/week)
100=Well-controlled (no symptoms)
1=Minor (mild hypertension)
5=Major (post-heart attack, heart failure)
Results
Awaiting CalculationEnter your details to see safety assessment
For years, doctors told people with asthma to avoid beta-blockers entirely. It wasn’t just a caution-it was a hard rule. But today, that rule is changing. If you have asthma and also need a beta-blocker for heart trouble, you’re not out of options. The key isn’t avoiding them completely-it’s choosing the right one and using it the right way.
Why Beta-Blockers Were Once Forbidden in Asthma
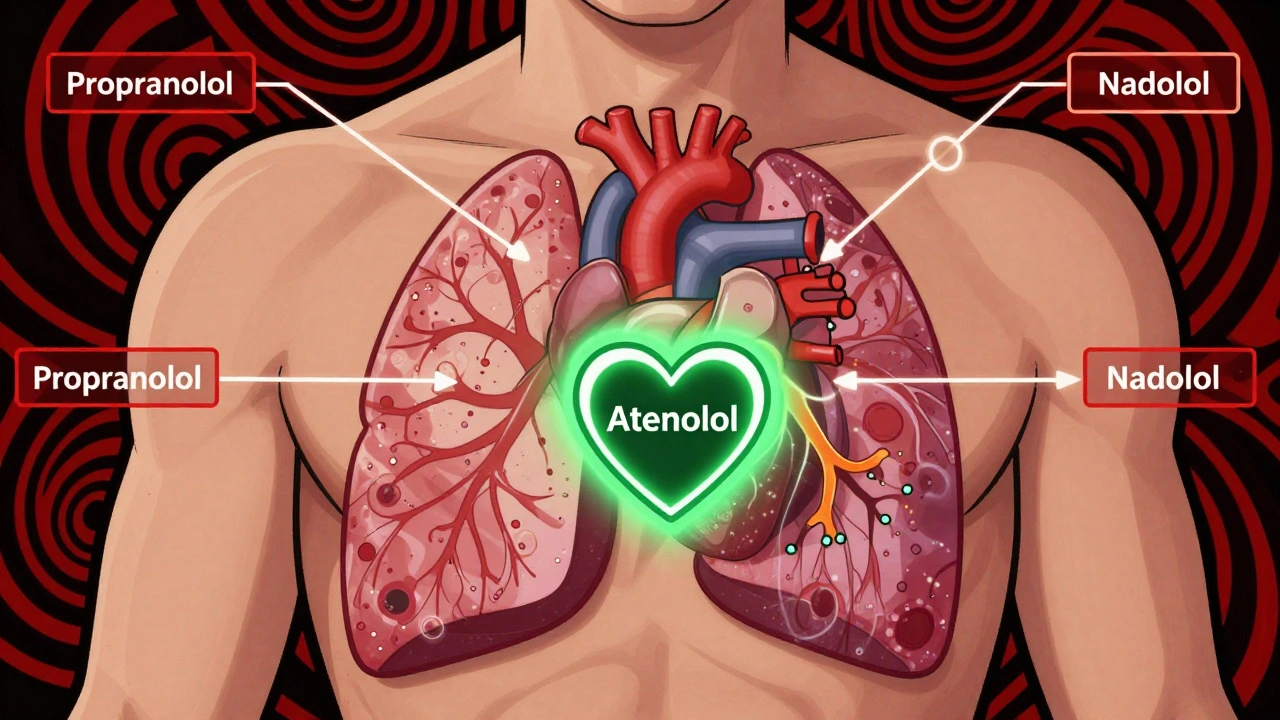
Beta-blockers work by slowing down your heart and lowering blood pressure. They’re lifesavers after a heart attack, for heart failure, or when you have high blood pressure. But they also block beta receptors in your lungs. Older beta-blockers like propranolol and nadolol hit both heart and lung receptors equally. That’s the problem. In the lungs, beta-2 receptors help keep your airways open. Block them, and your airways can tighten up-triggering wheezing, coughing, or even a full asthma attack. This isn’t theoretical. In the 1970s and 80s, asthma patients on these drugs did have more breathing problems. Some even ended up in the ER. So guidelines said: don’t use beta-blockers in asthma. Full stop.Not All Beta-Blockers Are the Same
Here’s the shift: not all beta-blockers are created equal. Today, we have two main types:- Non-selective beta-blockers - block beta-1 (heart) and beta-2 (lungs) receptors equally. Examples: propranolol, nadolol, timolol. These are still risky for asthma.
- Cardioselective beta-blockers - mostly target the heart. They have much less effect on the lungs. Examples: atenolol, metoprolol, bisoprolol.
What the Science Says About Safety
A 2021 meta-analysis reviewed 29 clinical trials involving asthma patients who took cardioselective beta-blockers. Here’s what they found:- On average, FEV1 (a key measure of lung function) dropped by just 7.5% after a single dose-far less than the 10% drop seen with non-selective versions.
- That drop was fully reversed by a rescue inhaler like albuterol.
- After weeks of daily use, no patient had worsening asthma symptoms or more attacks.
- Even when researchers induced mild bronchoconstriction, patients on cardioselective beta-blockers responded just as well to their inhalers as those not on the drugs.
Atenolol: The Top Choice for Asthma Patients
If you need a beta-blocker and have asthma, atenolol is currently the best-studied and safest option. It’s highly cardioselective, doesn’t cross the blood-brain barrier (which reduces side effects like fatigue), and has been used safely in asthma patients for decades. A 2023 review in the European Journal of Clinical Pharmacology specifically recommended atenolol for asthma patients needing beta-blockade-especially when paired with a regular beta-2 agonist inhaler. That’s not just theory. Real-world data from 330 asthma patients on cardioselective beta-blockers showed zero reports of fatal bronchospasm or severe respiratory events.
When Is It Safe to Use Them?
This isn’t a green light for everyone. You need to meet three criteria:- Your asthma is well-controlled. No recent hospital visits, no frequent rescue inhaler use.
- You have a strong cardiac reason for the beta-blocker-like after a heart attack, or with heart failure. The heart benefit must outweigh the lung risk.
- You’re under specialist care. A cardiologist or pulmonologist should start you on the lowest possible dose and monitor you closely.
What to Watch For
Even with the safest options, you need to stay alert:- Watch for new or worsening wheezing, shortness of breath, or chest tightness in the first 1-2 weeks.
- Keep your rescue inhaler with you at all times-even if you rarely use it.
- Don’t stop your inhaler just because you’re on a beta-blocker. You still need it.
- Get a lung function test (FEV1) before starting and again after 2-4 weeks.
What About Other Medications?
Some beta-blockers are still off-limits:- Labetalol - blocks alpha and beta receptors. Can cause airway tightening. Avoid.
- Propranolol, nadolol, timolol - non-selective. High risk. Don’t use.
- Carvedilol - has some beta-2 blocking effect. Not recommended for asthma.

Long-Term Effects: It Gets Better
Here’s the surprising part: the longer you take a cardioselective beta-blocker, the safer it seems. Animal studies show that while the first few days might slightly increase airway sensitivity, after weeks or months, inflammation in the airways actually goes down. That’s right-long-term use may have an anti-inflammatory effect in the lungs. One study found that celiprolol, a less common beta-blocker, didn’t just avoid causing bronchospasm-it actually blocked the airway-constricting effects of propranolol. That’s not just safe. That’s protective.Real-Life Scenarios
Imagine two people:- Person A - 62, had a heart attack 6 months ago, has mild asthma controlled with a daily inhaler. Their cardiologist prescribes atenolol 25 mg daily. They get a lung test before starting. Two weeks later, their FEV1 is unchanged. No wheezing. They’re back to walking daily without shortness of breath.
- Person B - 58, uses their rescue inhaler 3-4 times a week, has had two ER visits in the past year. Their doctor decides against beta-blockers and uses a different class of heart medication.
What’s Next?
The medical world is moving away from blanket bans. We now know that for many asthma patients, the risk of not treating heart disease is far greater than the risk of using a carefully chosen beta-blocker. Future research will focus on even more selective drugs and how long-term use might reduce airway inflammation. But for now, the message is clear: if you have asthma and heart disease, you don’t have to choose between your heart and your lungs. You just need the right drug, the right dose, and the right team watching over you.Can I take beta-blockers if I have asthma?
Yes-but only certain types. Cardioselective beta-blockers like atenolol, metoprolol, or bisoprolol can be safe if your asthma is well-controlled and you’re under specialist care. Non-selective ones like propranolol are still dangerous.
Is atenolol safe for asthma patients?
Yes. Atenolol is the most studied and safest cardioselective beta-blocker for people with asthma. Clinical trials show minimal impact on lung function, no increase in asthma attacks, and full responsiveness to rescue inhalers.
Will beta-blockers make my inhaler less effective?
Non-selective beta-blockers can reduce the effect of rescue inhalers like albuterol. Cardioselective ones like atenolol do not. Studies confirm that asthma patients on these drugs still respond normally to beta-agonists when they need them.
What should I do if I start wheezing after starting a beta-blocker?
Use your rescue inhaler immediately. Then contact your doctor. Don’t stop the medication on your own-your doctor may switch you to a different beta-blocker or adjust your asthma treatment. Never ignore new breathing symptoms.
Can I stop my beta-blocker if I’m worried about my asthma?
No. Stopping a beta-blocker suddenly-especially after heart surgery or for heart failure-can cause dangerous spikes in blood pressure, irregular heartbeat, or even another heart attack. Always talk to your doctor before making any changes.
Are there alternatives to beta-blockers for asthma patients with heart disease?
Yes. Calcium channel blockers like amlodipine or diltiazem, or ACE inhibitors like lisinopril, are often used instead. But they don’t offer the same protection after a heart attack. Beta-blockers remain the gold standard for post-heart attack care-so switching isn’t always better. The goal is finding the safest beta-blocker, not avoiding them entirely.
9 Comments
Robert Gilmore December 1, 2025 AT 20:15
whoa this is wild 😮 i always thought beta-blockers were a hard no for asthma folks. turns out it’s not the drug-it’s the *kind* of drug. atenolol sounds like the chill uncle of beta-blockers 🤝
Robert Gilmore December 2, 2025 AT 16:16
usa doctors still playing catch up? in europe they’ve been using cardioselective beta-blockers for asthmatics since the 90s. we dont need american guidelines to tell us what works. #medicinewoke
Robert Gilmore December 4, 2025 AT 10:36
the key here is receptor selectivity and dose dependency. non-selective agents like propranolol have high affinity for both beta-1 and beta-2 receptors which explains the bronchoconstriction risk. cardioselective ones like metoprolol and atenolol have >100:1 selectivity ratio for beta-1. but even then, individual variability matters-some asthmatics still react. that’s why titration and spirometry monitoring are non-negotiable
Robert Gilmore December 4, 2025 AT 21:33
the data is statistically significant but clinically trivial. a 7.5% drop in fev1 might be ‘reversible’ with albuterol, but that’s still a measurable physiological insult. and let’s not ignore the placebo effect in long-term studies-patients who know they’re on a ‘safe’ drug may subconsciously report fewer symptoms. the real risk isn’t bronchospasm-it’s the normalization of compromise in clinical decision-making. if we keep diluting guidelines, we’ll end up with a generation of patients who don’t know what ‘contraindicated’ even means
Robert Gilmore December 5, 2025 AT 18:16
i have asthma and take metoprolol. i’ve been on it for two years. no issues. i keep my inhaler nearby just in case. but honestly? i forget it’s even there. this post made me feel seen.
Robert Gilmore December 6, 2025 AT 09:10
so many people scared of meds these days 😅 but this makes sense. heart first, lungs second, but not ignoring either. atenolol sounds like the quiet hero here 🙌
Robert Gilmore December 8, 2025 AT 02:50
big pharma pushed this. they made the old ones illegal so they could sell the new ones. don’t trust the doctors. they’re paid off.
Robert Gilmore December 9, 2025 AT 13:16
it’s beautiful how medicine evolves from fear to nuance. once we saw beta-blockers as monsters in the lungs, now we see them as quiet guardians of the heart-with a few caveats. atenolol isn’t just safe-it’s poetic. a molecule that listens to both the heart’s cry and the lungs’ whisper, and chooses balance. who knew chemistry could be so tender?
Robert Gilmore December 10, 2025 AT 00:48
the evolution of clinical guidelines reflects the maturation of evidence-based practice. this transition from blanket contraindications to risk-stratified prescribing exemplifies precision medicine. the emphasis on specialist oversight, baseline pulmonary function testing, and concurrent beta-agonist use demonstrates a paradigm shift from dogma to individualized care. it is both scientifically rigorous and ethically responsible.